The Hippocratic Oath | Falling-action
A practical approach to handling a medical dilemma
(Fictional narrative by the doctor)
James Fleck, MD, PhD & João A de Andrade
Anticancerweb 08 (05), 2019
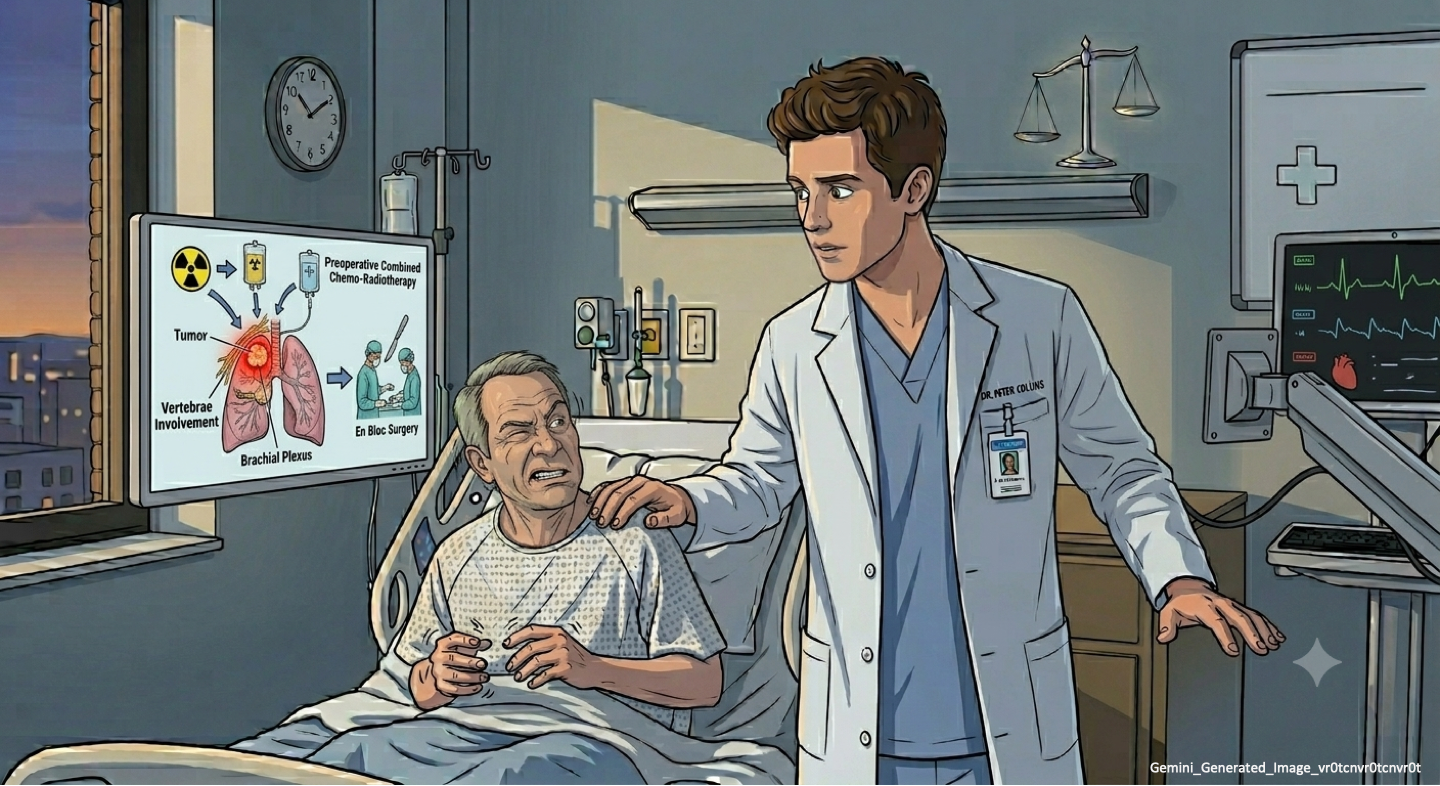
Before we started our morning rounds, Peter asked to talk to me. He was determined to take care of Edgar, but he had never cared for a patient with Tourette’s. He overcame his prejudice but was not satisfied with the quality of the physician-patient relationship. He sensed a communication gap. Although he felt that he had explained all the details about the clinical presentation of a Pancoast tumor, Edgar had an unexpected and somewhat bizarre verbal reaction. Peter was seeking my advice on how to communicate with Edgar in an effective way.
I suggested that a good first step would be for him to learn more about Tourette’s by reviewing the available literature. I was hoping that in doing so, he would realize that other medical professionals face exactly the same challenges he was dealing with.
The inability to communicate effectively is the root of the anti social behavior that is often associated with Tourette’s. Peter would have to understand that it is a neurological disease with unpredictable behavioral changes, associated with anxiety, involuntary muscle contractions and compulsive speech. Ultimately, I hoped that he realized that there was a dissociation between Edgar thoughts and what he was verbalizing.
Peter was a sensitive and affectionate doctor, and I was confident that he would learn to communicate with Edgar. As our conversation went on, Peter also brought up the social and economic challenges that could affect Edgar’s treatment plan.
Edgar's tumor was not yet fully staged. We were waiting for the results of the PET-CT and he also needed to have a mediastinoscopy to sample the lymphnodes that are located between the lungs. Analysis of the initial biopsy material had already revealed the tumor molecular profile, which was negative for EGFR mutation and ALK translocation. However, there was a 10% positive immunostaining for PD-L1, which suggested the potential for benefit with immunotherapy. Treatment with immunological checkpoint inhibitors has been shown to restore tumor cell immunity so one’s immunological system participates in the killing of the tumor. This finding was very significant and was recognized with the 2018 Nobel Prize in Medicine.
If Edgar's tumor was locally advanced (based on the presence of tumor cells in the mediastinal lymph nodes = “N2”disease), surgery would not be an option. He would be treated with chemoradiotherapy and we could potentially offer him consolidation immunotherapy with durvalumab. In the U.S., the PACIFIC trial showed an improvement in progression-free survival and 2-year survival with durvalumab consolidation treatment. An analytical microsimulation model developed at the Massachusetts General Hospital projected that the total cost of consolidation treatment with durvalumab would be approximately US$ 200,000, which in terms of cost-effectiveness would represent an increment of approximately US$ 67,000 per quality-adjusted life year (ICER/QALY = US$ 67,421.00). Prospectively, the model suggests economic viability in the US, where the GDP per capita is approaching US$ 70,000. If Edgar had any evidence of metastatic disease, the total cost of the sequential use of immunotherapy, chemotherapy, and palliative care would be about US$ 180,000, which is a prohibitive cost in low and middle income countries.
I warned Peter that he was thinking of a broad scenario and trying to deal with three hypotheses simultaneously:
Hypothesis 1: Pancoast tumor - stage IIIA (T3N1M0) characterized by invading the chest wall (T3), showing a positive hilar lymph node (N1), no disease in the mediastinum and a PET-CT negative for metastases (M0). Edgar would have a resectable disease. His treatment would include combined induction chemoradiotherapy, followed by surgery and consolidation chemotherapy. There would be no indication for durvalumab. It would be a low-cost treatment with curative intent.
Hypothesis 2: Pancoast tumor - stage IIIB (T3N2M0) characterized by invading the chest wall (T3), showing mediastinal disease (N2) with no distant metastases on PET-CT (M0). Edgar would have an unresectable tumor, which meant that he would not be treated with surgery. His treatment would include combined definitive chemoradiotherapy, followed by consolidation with durvalumab. It would be a high cost treatment with curative intent.
Hypothesis 3: Pancoast tumor - stage IV (T3N1M1) characterized by invading the chest wall (T3), showing positive hilar lymph node (N1) and presence of distant metastases on PET-CT (M1). Edgar would have no chance for cure. His treatment would include first-line immunotherapy (pembrolizumab), followed by chemotherapy on relapse (second-line treatment) and palliative treatment after progression. It would be a high cost treatment with palliative intent.
I told Peter that I could understand his concern! However, we should not handle all variables simultaneously. We would have to think sequentially. First, Peter had to be sure that he was no longer identifying Edgar with his brother's aggressor. Second, Peter would have to understand that Edgar’s Tourette’s will make communication more challenging. Third, the staging was not complete and the treatment plan was still undefined.
The cost associated with newly developed medical treatments is a worldwide problem. Novel and sophisticated interventions are usually very expensive, thereby stressing even more healthcare systems that are often already cash strapped. Society is largely unprepared to deal with these issues and attempts have been made to create formulas to better define whether a new treatment is either affordable and/or cost-effective.
In Oncology, the ICER/QALY ratio is used to evaluate the potential of a new drug as standard treatment. It is believed that the ratio should be below 2.5 times the per capita GDP (2.5 GDP) to justify a drug becoming the standard of care. In low income countries, without a robust public health system, a treatment cost that exceeds the limit of 2.5 GDP would benefit an individual but would limit resources for basic care such as vaccines and sanitation. The decision is complex and involves many stakeholders.
As we arrived at Edgar’s room, I asked Peter to let me lead the conversation. He agreed, but did so reluctantly!
Edgar was calm. The pain had been under control for the last 24 hours. Edgar was looking at a small chessboard, the only belonging that he was allowed to bring from prison. He was moving the pieces on either side, as if he were playing with an imaginary friend, without paying much attention to our presence.
I asked him where he learned to play chess.
He gave me a brief glance while telling me that he was a student of chess since he was a young child and played all the time. He felt less anxious when he played and only recently stopped when the pain became unbearable.
I asked if this was a good time for us to talk about his disease and his treatment options.
Edgar nodded, without looking away from the chessboard.
I began by asking him if he had any questions.
Edgar stopped the game, pushed aside the chessboard, and blurted out a string of questions in rapid succession: Could you stop my pain? Am I going to have to do more tests? Do I have to have surgery? Aren’t chemotherapy and radiation just for those who are dying? I just want to be pain free ...
Peter looked at me with a confused expression.
I looked at Edgar and asked him how far was he able to plan his chess game after his opponent’s first movement.
He promptly replied!
He told me that after the first move he was able to understand his opponent’s thought process. After two or three more moves he was able to have a fairly good strategy lined up to win the game.
I told Edgar that his disease would be investigated and treated as if it were a game of chess. First, a fragment of the tumor was removed through a needle biopsy under the guidance of a chest computed tomography. This material had been examined in the laboratory and the result would help us choose the best treatment. This was the opening movement of our chess game.
I explained to him that if the staging tests suggested that his disease could be ressected, his treatment would have a curative intention. Once the results were available, I would give him additional information.
Edgar agreed and seemed reassured by my explanation!
He then looked at Peter and asked if he wanted to play chess!
Much to my surprise, Peter accepted the challenge! I left them alone and went on to continue my daily rounds.
A week went by…
Peter told me that he had lost all the chess matches he had played with Edgar in the last five days. He was impressed by his intelligence and quick reasoning skills.
Peter used the time they were playing chess to keep Edgar informed about the progress of the clinical investigation.
Peter explained that the biopsy revealed a tumor called “adenocarcinoma”. A positron emission tomography (PET-CT) was performed, checking the entire body. Fortunately, it excluded the presence of distant metastases. Usually, a negative PET-CT has a high predictive value for the absence of involvement of mediastinal lymph nodes. This would be confirmed prior to definitive surgery by a mediastinal lymph node sampling technique called mediastinoscopy. If the mediastinal lymph nodes were negative for cancer cells Edgar would be staged as “IIIA” and treated with curative intention. The chance for cure is usually not bad. First, he would receive two cycles of combined chemoradiotherapy, followed by surgery and two additional cycles of chemotherapy based on cisplatin doublets as it was recommended by the Intergroup Trial 0160. Although Pancoast tumor is a rare presentation of lung cancer, this combined treatment approach has been used in several international centers for about 25 years, showing effective and safe results.
Despite all the technical progress, there is still a surgical mortality rate of 2.4%. The use of preoperative chemoradiotherapy increases the chance of a complete resection (R0) and a complete pathologic remission (CRp), which is predictive of a greater chance of cure. Recent data updated from systematic reviews on trimodality therapy have shown a 5-year overall survival rate ranging from 40 to 50% for a stage IIIA Pancoast tumor. Although the chance is equivalent to a coin toss, it is considerably better than the overall cure rate for lung cancer (15%). In addition, this would be a low-cost treatment, since immunotherapy would not be necessary.
Fortunately, it seemed that Peter would be spared from having to deal with the so-called social and economic conflict!
Peter had also learned how to deal with Edgar's limitations. The compulsive manifestations of Tourette syndrome, no longer impressed him so much. He always expected the best time to inform Edgar about the steps of his evaluation and treatment. Now that Edgar was able to trust Peter, he became more engaged and began to ask questions about the nature of the disease, the risks of treatment and the chances of cure.
Edgar was a lonely man. He never married, had no children, and his parents were already dead. He had no one to share his decisions with, except his physicians. This gave us an increased sense of ethical responsibility and we were mindful of the potential challenges involved with conducting the informed consent process with someone who is a prisoner.
We requested neurological and psychiatric assessments to ensure that Edgar had the necessary cognitive and emotional capability to engage in shared decision-making. He followed all our explanations attentively, and asked appropriate questions about risks and benefits. He seemed reassured when we told him that Peter and I believed that we were offering him the treatment with the best chance of success.
Edgar reflected for a few hours and finally agreed with the six-month long treatment plan that we proposed .
After the induction chemoradiotherapy there was an excellent clinical response and the follow up PET-CT was negative in the primary tumor area, hilar and mediastinal lymph nodes. Surgery then followed. The procedure was an en bloc resection of the upper lobe of the left lung that included the chest wall, using a posterior approach technique (Paulson). The histopathology demonstrated a complete histological response, which means that there was no residual cancer. The pain progressively reduced in intensity during the treatment and disappeared completely three weeks after surgery. The absence of pain was the main supporting argument for Edgar to continue to follow the treatment plan. There were several complications related to chemotherapy and radiotherapy, including mucositis in the mouth and esophagus and two episodes of febrile neutropenia treated with antibiotics and G-CSF, a colony-stimulating factor that helps with leukocyte count recovery.
This was definitely a great outcome.
There was a feeling of double healing.
Peter overcame his ethical dilemma and Edgar survived a Pancoast tumor!
To be continued in PLOT 6…
* Attention: The story 3 will be published sequentially from PLOT 1 to PLOT 6 and you will always see the most recent posting. To read Story 3 from the beginning, just click in the numbered links located at the bottom of the homepage.
© Copyright 2019 Anticancerweb
James Fleck, MD, PhD: Full Professor of Clinical Oncology at the Federal University of Rio Grande do Sul, RS, Brazil 2019 (Editor)
Joao A. de Andrade, MD: Professor of Medicine and Chief Medical Officer, Vanderbilt Lung Institute, Vanderbilt University Medical Center, Nashville, TN – USA 2019 (Associate Editor)
Please login to write your comment.
If you do not have an account at Anticancerweb Portal, register now.