The Smart Use of Two Humanized Monoclonal Antibodies (MoAb)
James F Fleck, MD, PhD
Anticancerweb 01 (05), 2021
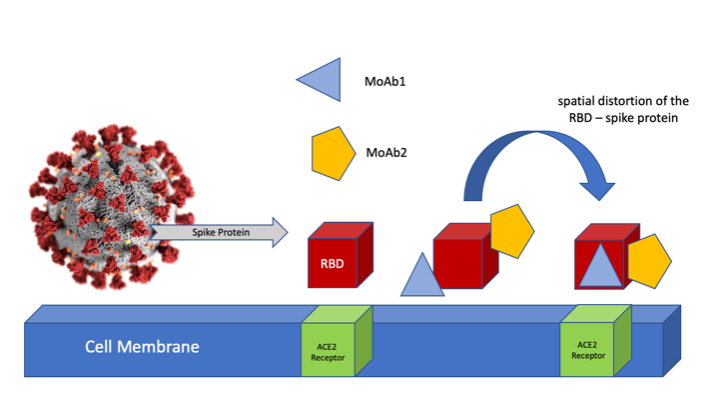
The biological mechanism of SARS-COV2 infection is well known. The receptor-binding domain (RBD) of the spike protein presented in the surface of SARS-COV2 binds to the angiotensin-converting enzyme-2 (ACE2)-receptor found in the host target cell membrane. Highly potent humanized-monoclonal antibodies have been developed to target non-overlapping specific epitopes of the viral RDB-spike protein. The combined use of two high affinity neutralizing monoclonal antibodies, might be an effective treatment against COVID-19. The strategy could also protect against emerging resistance due to viral mutation eventually induced by selective pressure associated to single MoAb treatments. The double MoAb blockade would cause a spatial distortion of the RDB-spike protein, making it no longer suitable for promoting effective binding to ACE2 receptor. This would decrease the ability of the virus to enter the target cell, which could be measured by reducing the host's viral load. The figure below is a rough artistic sketch to illustrate the reasoning that supports the MoAb double blockade.
 Recently, Regeneron Pharmaceuticals and Roche launched REGEN-COV, a cocktail composed by casirivimab (REGN10933) and imdevimab (REGN10987), MoAb directed to different and non-overlapping epitopes of the SARS-Cov2 RDB-spike protein. MoAb were developed from humanized mice and sera of patients recovered from COVID-19, showing high affinity binding (Kd = 37.1 to 42.8 pM) in competitive binding assays. Hydrogen deuterium exchange mass spectrometry (HDXMS) and single-particle cryo-electron microscopy were used, revealing where each MoAb contacts the surface of RDB. A three-dimensional (3D) reconstruction map showed that casirivimab (REGN10933) binds at the top of the RBD, extensively overlapping the binding site for ACE2, whereas the epitope for imdevimab (REGN10987) is located on the side of the RBD, away from the REGN10933 epitope, and has little to no overlap with the ACE2 binding site. The combined use of casirivimab and imdevimab caused antibody-mediated cytotoxicity and cellular phagocytosis in virally infected cells in vitro. Using well-designed animal models, REGEN-COV was associated to a decrease on viral load as well as a reduction in the incidence and severity of lung disease, when compared to placebo. An accelerated phase I,II and III placebo-controlled clinical trial was conducted in non-hospitalized symptomatic patients within the 3 days after positive molecular diagnosis and within 7-days of the first symptoms. Combined use of casirivimab and imdevimab was associated with a significant reduction (P < 0.0001) in baseline viral load (-0.36 log10 copies / ml), specially obtained in the higher viral load patients, who were seronegative at baseline. Additionally, a lower number of patients treated with combined MoAb had COVID-19-related hospitalizations or visits to emergency room facilities (H-VERF). The absolute risk reduction was more pronounced in patients with comorbidities (H-VERF was 3% with MoAb treatment x 9% in placebo.On March 10, 2021 Eli Lilly and Company announced the combined use of bamlanivimab and etesevimab MoAb against SARS-CoV2. Early treatment of COVID-19-high-risk ambulatory patients with combined bamlanivimab and etesevimab significantly decreased viral load compared with placebo at day 3 to day 11. In placebo-controlled phase III trial, the combined use of bamlanivimab and etesevimab was associated with 70% reduction in COVID-19 related hospitalization and deaths.
Recently, Regeneron Pharmaceuticals and Roche launched REGEN-COV, a cocktail composed by casirivimab (REGN10933) and imdevimab (REGN10987), MoAb directed to different and non-overlapping epitopes of the SARS-Cov2 RDB-spike protein. MoAb were developed from humanized mice and sera of patients recovered from COVID-19, showing high affinity binding (Kd = 37.1 to 42.8 pM) in competitive binding assays. Hydrogen deuterium exchange mass spectrometry (HDXMS) and single-particle cryo-electron microscopy were used, revealing where each MoAb contacts the surface of RDB. A three-dimensional (3D) reconstruction map showed that casirivimab (REGN10933) binds at the top of the RBD, extensively overlapping the binding site for ACE2, whereas the epitope for imdevimab (REGN10987) is located on the side of the RBD, away from the REGN10933 epitope, and has little to no overlap with the ACE2 binding site. The combined use of casirivimab and imdevimab caused antibody-mediated cytotoxicity and cellular phagocytosis in virally infected cells in vitro. Using well-designed animal models, REGEN-COV was associated to a decrease on viral load as well as a reduction in the incidence and severity of lung disease, when compared to placebo. An accelerated phase I,II and III placebo-controlled clinical trial was conducted in non-hospitalized symptomatic patients within the 3 days after positive molecular diagnosis and within 7-days of the first symptoms. Combined use of casirivimab and imdevimab was associated with a significant reduction (P < 0.0001) in baseline viral load (-0.36 log10 copies / ml), specially obtained in the higher viral load patients, who were seronegative at baseline. Additionally, a lower number of patients treated with combined MoAb had COVID-19-related hospitalizations or visits to emergency room facilities (H-VERF). The absolute risk reduction was more pronounced in patients with comorbidities (H-VERF was 3% with MoAb treatment x 9% in placebo.On March 10, 2021 Eli Lilly and Company announced the combined use of bamlanivimab and etesevimab MoAb against SARS-CoV2. Early treatment of COVID-19-high-risk ambulatory patients with combined bamlanivimab and etesevimab significantly decreased viral load compared with placebo at day 3 to day 11. In placebo-controlled phase III trial, the combined use of bamlanivimab and etesevimab was associated with 70% reduction in COVID-19 related hospitalization and deaths.The four MoAb are among the most potent SARS-CoV2 neutralizing antibodies in use or in clinical development. However, concerns have been raised about its effectiveness against the Brazilian P1 variant, which increases the importance of full vaccination coverage.
References:
1. Jun Lan, Jiwan Ge, Jinfang Yu, et al: Structure of the SARS-CoV-2 spike receptor-binding domain bound to the ACE2 receptor, Nature 581: 215-220, May 14th, 2020
2. Johanna Hansen, Alina Baum, Kristen E. Pascal, et al: Studies in humanized mice and convalescent humans yield a SARS-CoV-2 antibody cocktail, Science 369, 1010–1014, August 21st, 2020
3. Zhiqiang Ku, Xuping Xie, Edgar Davidson, et al: Molecular determinants and mechanism for antibody cocktail preventing SARS-CoV-2 escape, Nature Communications, 2021 (https://doi.org/10.1038/s41467-020-20789-7)
4. Peter C. Taylor, Andrew C. Adams, Matthew M. Hufford, et al: Neutralizing monoclonal antibodies for treatment of COVID-19, Nature Reviews – Immunology, 2021
5. Alina Baum, Benjamin O. Fulton, Elzbieta Wloga, et al: Antibody cocktail to SARS-CoV-2 spike protein prevents rapid mutational escape seen with individual antibodies, Science 10.1126 science.abd0831, 2020
6. Roche Communication: New phase III data shows investigational antibody cocktail casirivimab and imdevimab reduced hospitalization or death by 70% in non-hospitalized patients with COVID-19, March 23rd, 2021
7. D.M. Weinreich, S. Sivapalasingam, T. Norton, et al: REGN-COV2, a Neutralizing Antibody Cocktail, in Outpatients with Covid-19, N Engl J Med 384:238-51, 2021
8. Eli Lilly Communication: Lilly's bamlanivimab and etesevimab together reduced hospitalizations and death in Phase 3 trial for early COVID-19, March 10th, 2021
9. Pengfei Wang, Ryan G. Casner, Manoj S. Nair, et al: Increased Resistance of SARS-CoV-2 Variant P.1 to Antibody Neutralization, bioRxiv, version posted April 9, 2021, DOI: https://doi.org/10.1101/2021.03.01.433466
10. Photo by CDC (modified)
Authors Info & Affiliations:
James Fleck, MD, PhD: Full Professor of Clinical Oncology at the Federal University of Rio Grande do Sul, RS, Brazil (www.jamesfleck.com)
® Anticancerweb Copyright 2018
Interesting editorial, and shows a promising path for the treatment of COVID. Antibodies are an efficient and fast way to treat viral diseases, with an accelerated development with the new technologies of production of antibodies, such as "phage display". The big challenge is to identify even viral sites that are important in virulence. I believe that the production of antibodies that act on ACE2 receptors has been shown to be the most logical path for promising treatments, mainly by preventing the entry of the sars-cov-2 virus into cells, it is also a highly conserved region, which leads to safety for the application of drugs against the new variants
Please login to write your comment.
If you do not have an account at Anticancerweb Portal, register now.